In our last Blog, we discussed the impact of the presence of Bacterial Fluorescence (Biofilm) on Split Thickness Skin Graft Survival Rates and Wound Size Demographics. And keeping in tempo with Wound Bed Preparation, I would like to share the “how” in the eradication of Biofilm from the wound bed.
The slides presented are from Dr. Andrew Rader, a well renowned physician, researcher, and KOL in Biofilm, and a dear personal colleague. Earlier this year, Dr. Rader conducted a small preliminary study on the efficacy of Biofilm removal using the EZDebride Wound Instrument vs a standard Surgical Curette.
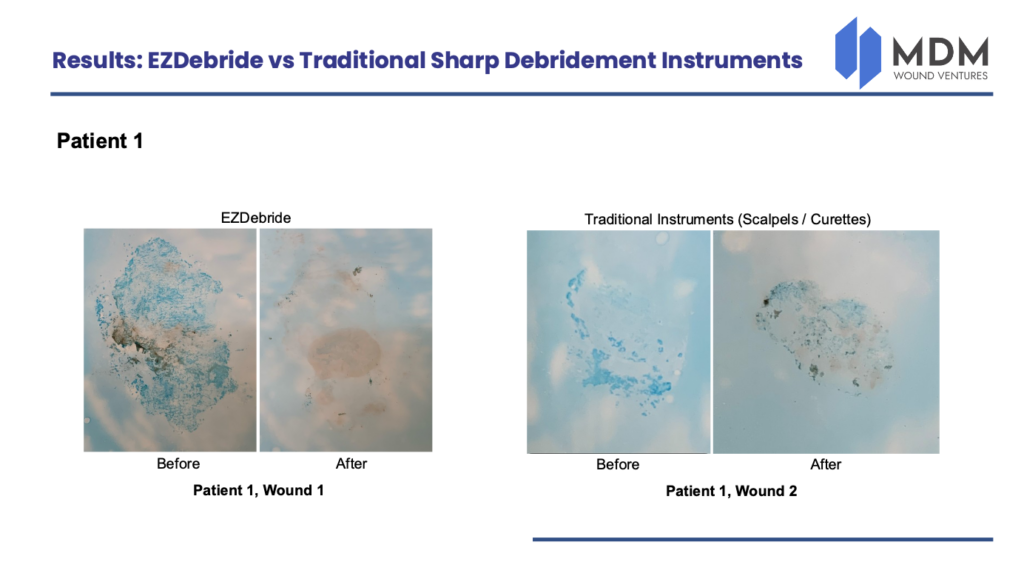
PATIENT 1: In this example, Alcian Blue Staining was used to identify Biofilm prior to sharp debridement in both wounds. Wound 1 was sharply debrided using an EZDebride Wound Instrument while Wound 2 was sharply debrided using a Curette. Following, the wounds were then stained again. In the first wound, note almost total eradication of the Biofilm with the EZDebride and conversely, note the increase in Biofilm remaining (and more) in the second wound with the Curette. Interestingly, you may be wondering why does Wound 2 appear to have more Biofilm present following debridement? The answer is because Biofilm is layered within the wound, and current studies have revealed that Biofilm also survives below the wound. And with uncontrolled depth debridement using a Curette, along with complications of pain and bleeding, this may result in inadequate depth and area debridement and therefore exposing hidden colonies of Biofilm below the surface. Keep in mind, if using a Curette, and especially with patients on Anti-Coagulant medication, excessive bleeding and pain may preclude the wound to continued debridement thus leaving a multitude of Biofilm behind along with exposed colonies as demonstrated in this example. In fact, the EZDebride Wound Instrument has demonstrated more reproducible and repeatable results. For example, lets look and the Patient 2.
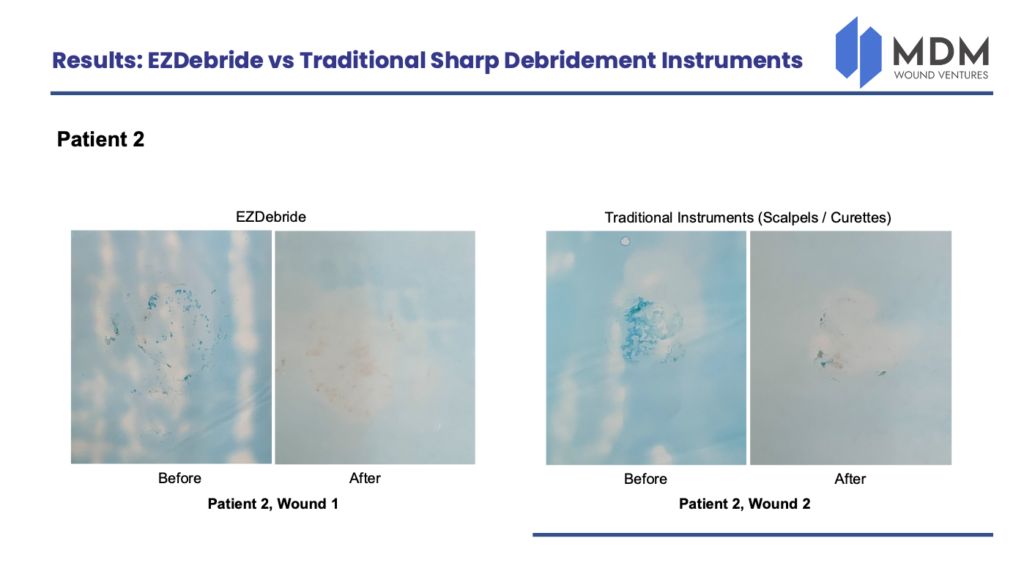
PATIENT 2: In examining Patient 2 Wound 1, please note again almost total if not complete eradication of the Biofilm. In Patient 2 Wound 2, again Biofilm is still present, however not to the extent in the first example. Again, the key takeaway is the fact that the EZDebride performs at a consistent level while the Curette demonstrates inconsistency. The question remains, can this preliminary study usher in a new methodology in the treatment of Biofilm? Perhaps, but you will have to wait until my next blog in which I will provide a detailed look of how it possibly can. Thank you again for tuning in and looking forward to our next post. Please check back next week and until the next time, fair winds and following seas.